CJC-1295
A growth hormone–releasing hormone analog best known for its Drug Affinity Complex, which binds albumin and extends GH/IGF-1 stimulation from minutes to days.
CJC-1295 at a glance
DAC and “no DAC” are not a minor formulation choice
CJC-1295 with DAC
- Modified GHRH sequence plus reactive Drug Affinity Complex
- Forms a covalent bond with circulating albumin
- Estimated half-life measured in days
- Studied in healthy adults using weekly or biweekly exposure
- Sustained GH trough and IGF-1 elevation
- Cumulative exposure after repeated dosing
“CJC-1295 without DAC”
- Usually a vendor name for Modified GRF(1-29)
- Also called Mod GRF or tetrasubstituted GRF(1-29)
- No albumin-binding DAC group
- Short action designed around discrete secretagogue pulses
- Often paired with ipamorelin
- Not the molecule tested in the famous long-acting human trial
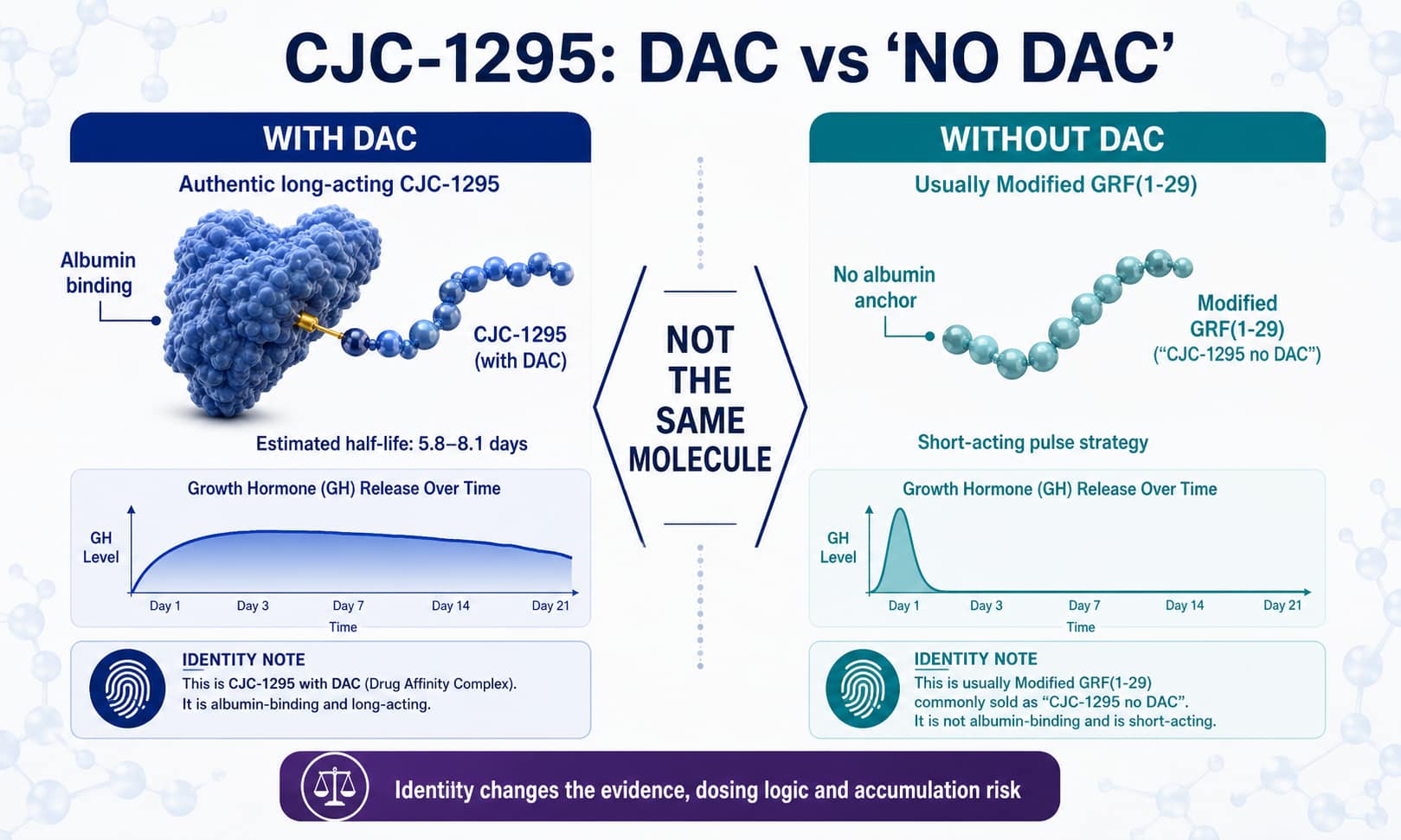
Suggested graphic: authentic DAC molecule versus Modified GRF(1-29) naming map · 1500 × 900
Long exposure without completely flattening GH pulses
Albumin anchoring
After injection, the DAC group reacts with albumin. Albumin acts as a circulating carrier, slowing clearance and proteolytic breakdown.
DAC-specificGHRH receptor
The active peptide stimulates pituitary somatotrophs, increasing endogenous growth hormone rather than supplying exogenous HGH.
Pituitary dependentPulses persist
A small human study found that pulsatility remained one week after DAC dosing, while GH troughs rose markedly. It did not simply create a flat GH infusion.
Human physiologyIGF-1 exposure
Longer GH stimulation raises hepatic IGF-1 for many days. Multiple DAC doses can accumulate before the earlier dose has fully cleared.
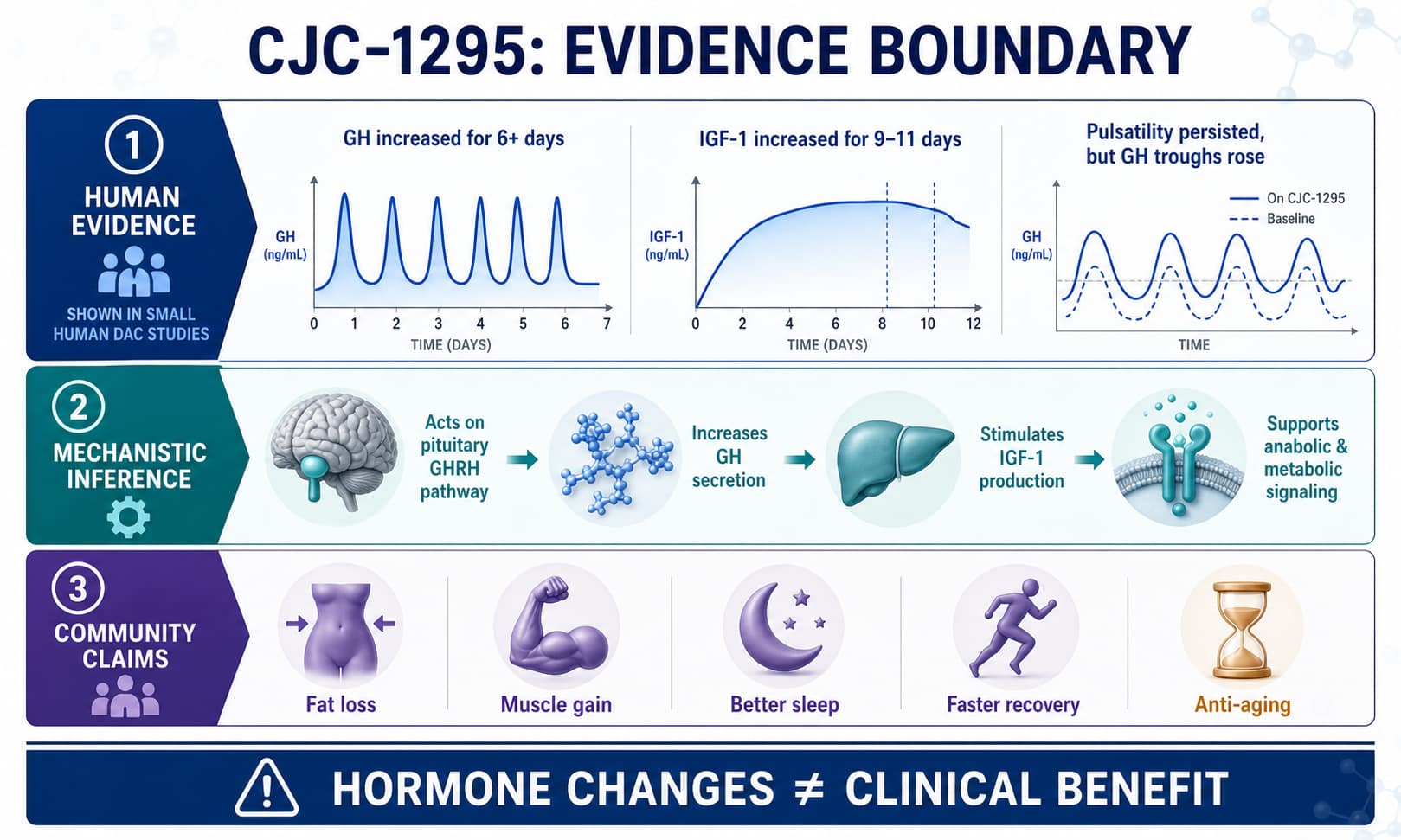
Monitoring concernStrong hormonal effects, weak outcome evidence
Healthy-adult hormone study
Two ascending-dose trials found dose-dependent GH increases of roughly 2–10 times baseline for at least six days and IGF-1 increases of roughly 1.5–3 times baseline for 9–11 days after one DAC injection.
GH pulsatility
Overnight sampling in healthy men one week after DAC showed preserved pulses but substantially higher basal GH and a 45% rise in IGF-1.
Modified GRF(1-29) stacks
Short-acting “no DAC” schedules are based on GHRH biology, secretagogue synergy, and community experience. They were not tested in the published CJC-1295 DAC trials.
- No validated optimal ipamorelin ratio
- No controlled bodybuilding outcomes
- No established long-term safety
Body composition and anti-aging
There are no robust controlled trials showing that CJC-1295 produces meaningful fat loss, muscle gain, injury healing, better sleep, or healthspan extension in healthy adults.
- Hormone movement is a surrogate endpoint
- Higher IGF-1 is not synonymous with better aging
- Long-term cancer and metabolic outcomes are unknown
| Claim | Direct CJC-1295 evidence | Best interpretation |
|---|---|---|
| Raises GH | Yes, small controlled DAC studies | Well supported pharmacodynamically |
| Raises IGF-1 | Yes, lasting many days with DAC | Well supported; exposure can accumulate |
| Builds muscle | No controlled outcome trial | Plausible claim, not demonstrated benefit |
| Burns fat | No controlled body-composition trial | Cannot borrow tesamorelin outcomes |
| Improves sleep/recovery | No robust direct trial | Community reports only |
Suggested graphic: proven hormone effects versus unproven outcome claims · 1500 × 900
Two community strategies built around different kinetics
DAC protocols
- Common range: 1–2 mg once weekly
- Alternative: smaller amounts twice weekly
- Cycles: commonly 8–16 weeks
- Goal: sustained IGF-1 and fewer injections
- Stacking: sometimes paired with ipamorelin despite continuous GHRH exposure
- Main concern: accumulation and persistent high IGF-1
“No DAC” / Mod GRF protocols
- Common amount: 100 mcg per administration
- Frequency: one to three times daily
- Pairing: often 100 mcg ipamorelin in the same session
- Timing: bedtime, fasted morning, or post-training
- Food spacing: users often avoid meals around dosing
- Goal: discrete GH pulses with low background exposure
Separate long-acting milligrams from short-acting micrograms
Hypothetical weekly-use concentration.
More concentrated weekly reference.
Common pulse-oriented concentration.
Mod GRF vial
liquid
10 mcg per unit
Long action makes errors last longer
FDA has identified significant concerns
CJC-1295 is not FDA approved. FDA places it among bulk substances that may present significant safety risks for compounding, citing limited clinical data, immunogenicity and peptide-characterization concerns, and serious adverse events including increased heart rate and systemic vasodilatory reaction.
FDA’s review also raised nonclinical injection-site, DNA-damage, and theoretical pituitary-overstimulation concerns; long-term carcinogenicity data are absent.
Common questions about CJC-1295
Is CJC-1295 without DAC really CJC-1295?
Which form was studied in humans?
Does DAC eliminate GH pulses?
Why is no-DAC paired with ipamorelin?
Does CJC-1295 burn fat or build muscle?
Is CJC-1295 FDA approved?
Where this information comes from
Explore related roadmap pages
Know which molecule is actually in the vial.
With CJC-1295, DAC versus “no DAC” changes the identity, half-life, dosing logic, evidence base, and risk of accumulation—not just the injection schedule.
Explore the Research Library