NAD+
Nicotinamide adenine dinucleotide is an essential coenzyme used in energy transfer, redox chemistry, DNA-repair signaling, and cellular stress responses. Its biology is fundamental; that does not make commercial NAD+ infusions a proven anti-aging, energy, cognition, recovery, or “detox” treatment.
NAD+ at a glance
“NAD therapy” can mean five different things
Route, redox form, precursor, salt, concentration, excipients, and finished-product quality determine what was actually administered. Product names alone cannot establish equivalence.
NAD+
The oxidized form accepts electrons during metabolic reactions and is also consumed by enzymes such as PARPs, sirtuins, and CD38. Direct infusion studies examine this molecule or a salt of it.
NADH
The reduced form donates electrons, including to mitochondrial respiratory complex I. It has different chemistry and product behavior; oral NADH trials are not direct NAD+ infusion trials.
NR and NMN
These are biosynthetic precursors that cells can use to build NAD+. Many more human trials test oral NR or NMN than direct NAD+, but precursor target engagement does not prove a direct infusion outcome.
Finished product
“NAD+ 500 mg” does not disclose counterion, hydration state, assay basis, pH, sterility, endotoxin, particulate control, container stability, or whether the ingredient was drug-grade rather than food-grade.
The plus sign is chemistry, not marketing
NAD+ is reduced when it accepts a hydride equivalent and becomes NADH; NADH is oxidized when it transfers electrons back. This cycling helps couple fuel oxidation to ATP production, but simply adding extracellular NAD+ does not guarantee delivery to a chosen tissue or organelle.
Mass arithmetic has a hidden assumption
The commonly quoted 663.4 g/mol describes a defined NAD+ form. Disodium salts, hydrates, reduced NADH, and other forms have different molecular weights. A label should state the chemical form and whether milligrams refer to the salt or NAD+ equivalent.
Essential intracellular biology does not prove extracellular delivery
NAD+ sits at the intersection of metabolism and signaling. The important translational question is not whether cells need NAD+—they do—but whether a particular product, route, amount, schedule, and patient population produces a meaningful clinical outcome.
Redox metabolism
NAD+/NADH transfers reducing equivalents through glycolysis, the tricarboxylic-acid cycle, fatty-acid oxidation, and mitochondrial respiration. The ratio is compartment-specific rather than one universal “energy score.”
Consumed as substrate
PARPs use NAD+ during DNA-damage signaling; sirtuins use it during protein deacylation; CD38 and related enzymes cleave it in signaling pathways. These reactions generate different metabolites and have context-dependent effects.
Delivery problem
Large, charged NAD+ does not behave like a freely diffusing small molecule. Extracellular breakdown, transporters, tissue uptake, recycling, renal loss, and infusion rate can all shape exposure.
Compartment problem
Blood, muscle, liver, brain, cytosol, nucleus, and mitochondria maintain different NAD pools. A blood measurement cannot automatically prove mitochondrial or brain delivery.
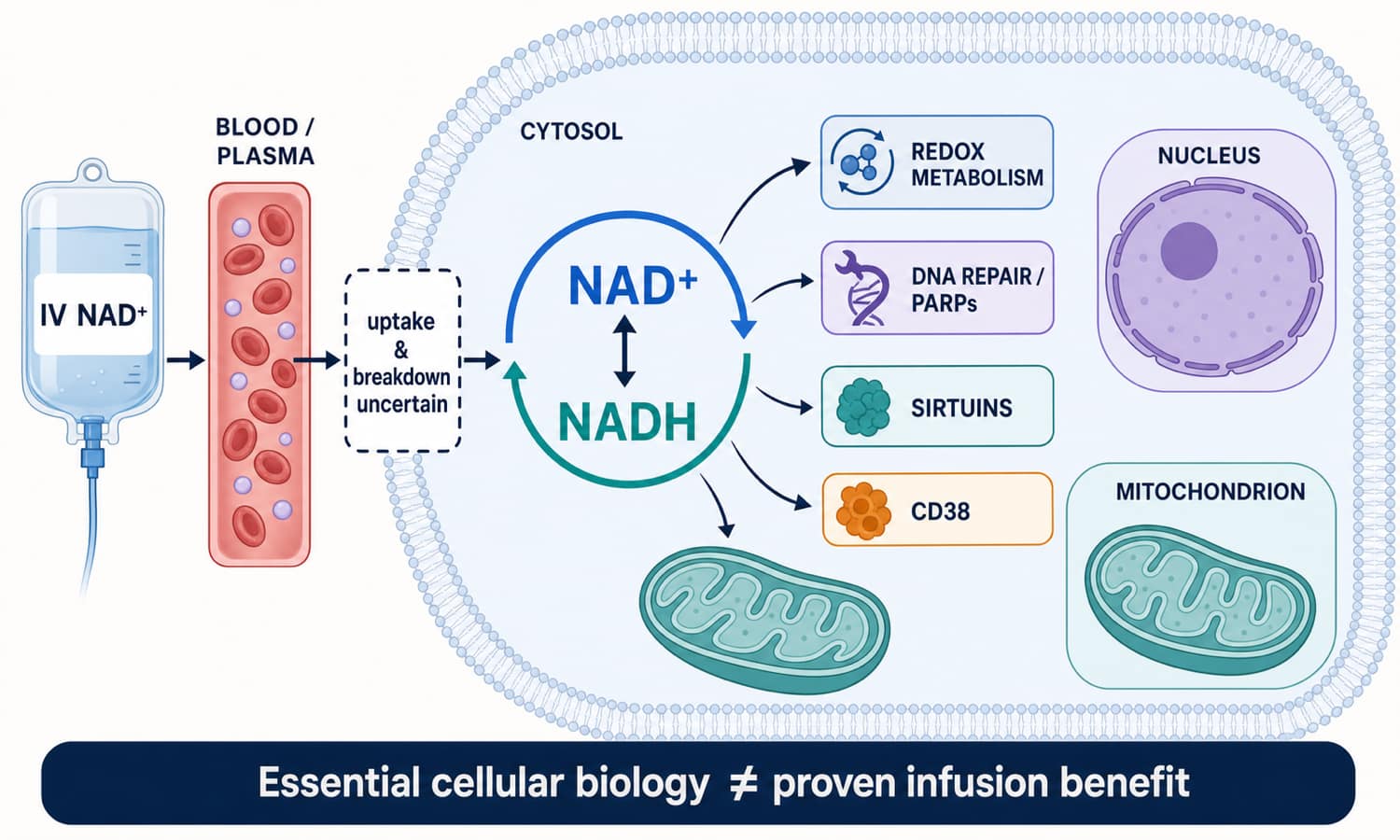
Planned image 1: NAD+ redox cycle, cellular roles, and delivery boundary map · 1500 × 900
What established biology supports
- NAD+ is essential for cellular redox reactions
- NAD+/NADH ratios vary by compartment and metabolic state
- PARPs, sirtuins, and CD38 consume NAD+
- Age, disease, inflammation, nutrition, and tissue type can affect NAD metabolism
- Direct infusion fate can be measured with plasma and urine metabolites
What it does not establish
- That more circulating NAD+ always improves cellular energy
- That an infusion reaches brain or mitochondrial NAD pools
- That a biomarker change reverses biological aging
- That direct NAD+, NR, NMN, NADH, and niacin are clinically equivalent
- That healthy people gain better cognition, sleep, performance, or lifespan
Direct NAD+ evidence is growing, but it is not a wellness outcome program
Recent direct-administration trials in heart failure and sudden hearing loss create legitimate research signals. They used low doses in specific hospital populations alongside standard care and cannot validate commercial high-dose anti-aging infusions.
| Evidence | Design and exposure | Main result | How to read it |
|---|---|---|---|
| Metabolism pilot Grant et al., 2019 | Eight healthy men received NAD+ at 3 μmol/min for six hours; three saline controls were also studied | Plasma NAD+ and measured metabolites did not rise for two hours; urinary NAD+ and methyl-nicotinamide increased by six hours; no observed adverse events | Tiny, nonrandomized pilot designed for metabolic fate, with no energy, cognition, recovery, aging, or disease outcome |
| Commercial review Reyna et al., 2026 | Retrospective records: six clients received 500 mg NAD+ in 500 mL saline on four consecutive days; eight received IV NR | All six NAD+ clients reported moderate-to-severe infusion symptoms; the average NAD+ infusion took about 97 minutes | Very small, nonrandomized commercial cohort with employee conflicts; useful tolerability warning, not an efficacy study |
| Disease RCT Ischemic heart failure, 2026 | Single-center, randomized, placebo-controlled trial; 180 adults; 10 mg/day IV for seven days plus guideline-directed therapy | One-month left-ventricular ejection fraction favored NAD+; six-month event and functional outcomes were nonsignificant trends | Promising disease-specific signal requiring multicenter replication; it does not test healthy aging or 500–1,000 mg clinic infusions |
| Disease RCT Sudden hearing loss, 2026 | Single-center double-blind trial; 45 randomized, 38 completed; low-dose injected NAD+ added to standard treatment | Three-month hearing improvement and recovery classifications favored the NAD+ group | Small adjunctive hospital study with attrition and a specific acute condition; not evidence for wellness, chronic tinnitus, or general neuroprotection |
| Uncontrolled series Substance-use treatment | Fifty difficult-to-treat patients received a proprietary NAD+-plus-enkephalinase-inhibition combination and completed symptom scales | Craving, anxiety, and depression scores decreased from baseline | No placebo group, multiple ingredients, subjective outcomes, and substantial expectancy/confounding; does not isolate NAD+ |
| Missing Healthy-aging outcomes | No adequate direct NAD+ trial program with long follow-up and validated healthspan endpoints | No established effect on lifespan, frailty, cognition, exercise performance, chronic fatigue, sleep, metabolic disease prevention, or “detoxification” | Biological plausibility and precursor studies do not fill this direct evidence gap |
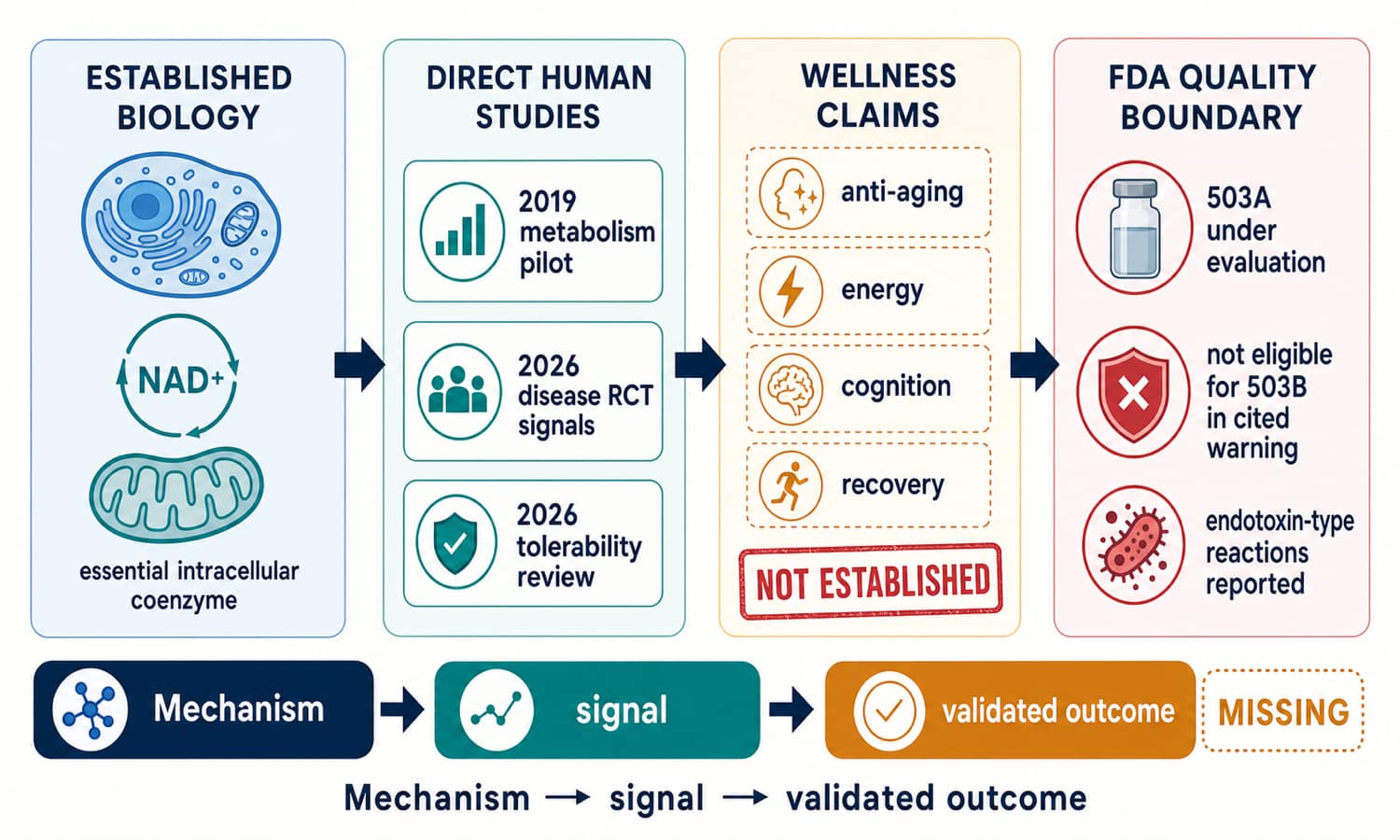
Planned image 2: NAD+ human evidence, wellness gap, and FDA compounding boundary map · 1500 × 900
Compounding categories are conditional pathways—not approvals
What is not established
- There is no FDA-approved IV NAD+ product for anti-aging, energy, cognition, recovery, addiction treatment, or wellness
- Compounded drugs are not FDA-approved and are not pre-reviewed like approved products for safety, effectiveness, or manufacturing quality
- An NDC listing, DailyMed entry, prescription, or clinic administration does not by itself mean FDA approval
- Food-grade or dietary-supplement ingredients are not automatically suitable for sterile drug compounding
503A versus 503B
FDA’s May 14, 2026 503A nomination document listed nicotinamide adenine dinucleotide in Category 1—substances under evaluation. That is not inclusion on a final positive bulks list. FDA’s January 2026 GenoGenix warning letter stated that NAD+ was not eligible for that outsourcing facility’s 503B bulk compounding because it was not on the 503B bulks list or used for a drug on the shortage list.
FDA safety reminder
FDA reported severe chills, shaking, vomiting, and fatigue after injectable NAD+; some patients needed medical treatment. The reactions were consistent with excessive endotoxin exposure.
Food-grade ingredient risk
FDA specifically warned that food-grade NAD+ can carry microbial and endotoxin risks and is not suitable for sterile compounding without appropriate drug-manufacturing controls.
Documented 2025 event
A 2026 warning letter described three patients sent to the emergency room after receiving NAD+ from one vial. An unopened vial from the same lot tested at 3,360 EU/mL bacterial endotoxin.
Category is not quality
Even when a substance is nominated or may be compounded under a legal pathway, each finished batch still needs appropriate identity, strength, sterility, endotoxin, particulate, stability, labeling, and dispensing controls.
Common protocols are conventions, not validated dosing
Wellness communities discuss NAD+ as a rapid “repletion” intervention for energy, mental clarity, jet lag, athletic recovery, aging, withdrawal, and post-illness fatigue. Controlled human trials do not establish these uses or an optimal blood level to target.
Entry-dose discussion
Often described as a first-session or tolerability range. It is not a validated minimum effective wellness dose, and IV product quality remains central at any amount.
Common clinic discussion
Frequently marketed over one to several hours. A 2026 retrospective review used 500 mg on four consecutive days and recorded moderate-to-severe infusion symptoms in all six NAD+ recipients.
High-dose discussion
Often promoted for “repletion,” longevity, or addiction protocols. No randomized wellness outcomes program validates the higher amount, cycle length, or claimed dose-response.
Common stacking conversations
| Stack discussion | Community rationale | Evidence boundary |
|---|---|---|
| NAD+ + glutathione | Pair redox-cofactor language with an antioxidant narrative | No controlled human combination study establishes superior energy, detoxification, recovery, or safety; separate infusions still share line and sterility risks |
| NAD+ + B vitamins | Supply nutrient precursors and cofactors alongside direct NAD+ | No validated formula, sequence, or deficiency-independent synergy; some vitamins can cause reactions at IV doses |
| NAD+ + MOTS-c | Combine cellular-redox and mitochondrial stress-signaling narratives | No human combination trial; direct NAD+ and MOTS-c have different identities, exposures, and evidence levels |
| NAD+ + SS-31 | Pair coenzyme replenishment claims with cardiolipin-focused mitochondrial biology | No validated synergy, timing, or safety program; SS-31’s narrow approved indication does not transfer to NAD+ wellness use |
| NAD+ + exercise or fasting | Attempt to amplify metabolic adaptation or “mitochondrial renewal” | No direct outcomes trial establishes better training adaptation; dehydration, low intake, or illness can worsen infusion tolerability |
If an intervention is being evaluated
- Define one measurable goal before the session
- Record product, lot, concentration, total volume, rate, duration, symptoms, and co-infusions
- Keep caffeine, sleep, training, hydration, and other interventions stable when practical
- Do not treat a transient flush or sensation as target engagement
- Do not infer brain or mitochondrial exposure from a nonspecific energy rating
Why anecdotes pull in both directions
Infusion time, expectation, hydration, saline volume, rest, clinic attention, concurrent vitamins, recovery from illness, and natural symptom fluctuation can create apparent benefit. Rate-related cramping or chest pressure can create apparent harm even without laboratory injury. Both observations deserve documentation; neither estimates efficacy alone.
Mixing math for a hypothetical 500 mg bag
This is label arithmetic, not an IV preparation, rate, or dosing instruction. Sterile compounding and administration require trained professionals, verified drug-grade ingredients, appropriate facilities, product-specific compatibility data, and clinical monitoring.
| Hypothetical pump rate | Bag duration | NAD+ rate at 1 mg/mL | Calculation |
|---|---|---|---|
| 50 mL/hour | 10 hours | 50 mg/hour | 500 mL ÷ 50; 50 × 1 |
| 100 mL/hour | 5 hours | 100 mg/hour | 500 ÷ 100; 100 × 1 |
| 125 mL/hour | 4 hours | 125 mg/hour | 500 ÷ 125; 125 × 1 |
| 250 mL/hour | 2 hours | 250 mg/hour | 500 ÷ 250; 250 × 1 |
| 500 mL/hour | 1 hour | 500 mg/hour | 500 ÷ 500; 500 × 1 |
Universal formulas
Amount ÷ final volume = concentration.
Volume ÷ pump rate = time.
Concentration × pump rate = amount per hour.
These relationships can check a label or order; they cannot supply a safe prescription.
High-risk error sources
- Confusing vial volume with final bag volume
- Using NADH, a sodium salt, or a hydrate as though it were the same NAD+ form
- Reading 500 mg/5 mL as 500 mg/mL instead of 100 mg/mL
- Changing rate to manage symptoms without clinical assessment
- Assuming saline dilution removes endotoxin or makes food-grade powder injectable
- Combining products in one bag without compatibility and stability data
No universal storage rule covers every NAD+ product
Use the exact label
Follow the dispensing source’s written temperature, light, container, dilution, in-use time, and beyond-use instructions. A dry powder, concentrated vial, pre-mixed bag, and oral product are different dosage forms.
Cold does not equal sterile
Refrigeration may slow some chemical degradation, but it cannot remove endotoxin, reverse microbial contamination, correct the wrong salt, or restore potency lost before dispensing.
Protect from stressors
Temperature, light, pH, oxygen exposure, repeated puncture, container surfaces, and time can affect a finished formulation. Product-specific stability data—not the NAD+ name—should set limits.
Appearance is incomplete
Cloudiness, particles, color change, leakage, or a damaged seal are stop signs. A clear solution can still contain excessive endotoxin, microbes, invisible particles, or the wrong concentration.
Separate molecule effects, rate effects, line risks, and batch quality
Reactions can be clinically significant
The 2026 retrospective commercial review recorded abdominal cramping, diarrhea, nausea, vomiting, increased heart rate, throat pain, congestion, and chest pressure during NAD+ infusion in all six recipients. Symptoms stopped when infusions ended, but the sample was too small to estimate frequency or rare risks.
FDA’s adverse-event reports add a different danger: severe chills, shaking, vomiting, and fatigue consistent with excessive endotoxin. A slower rate cannot make a contaminated batch safe.
Stop infusion and seek urgent care
- Chest pain or pressure, trouble breathing, throat tightness, facial swelling, or faintness
- Severe shaking chills, fever, confusion, rapidly worsening weakness, or low blood pressure
- Persistent vomiting or diarrhea, severe abdominal pain, or a sustained fast or irregular heartbeat
- Increasing IV-site pain, swelling, redness, streaking, leakage, tissue discoloration, or numbness
- Any cluster of reactions linked to the same vial, lot, clinic session, or co-infused product
Review before elective use
- Heart failure, kidney disease, uncontrolled blood pressure, rhythm disorder, or fluid restriction
- Pregnancy, breastfeeding, fertility treatment, or use in a child
- Active cancer, recent cancer therapy, or an unexplained mass
- Multiple IV ingredients, uncertain compatibility, or recent infusion reaction
- Food-grade starting material, missing lot traceability, or no sterility/endotoxin documentation
- Symptoms that need diagnosis rather than a wellness infusion
Common questions about NAD+
Is NAD+ a peptide?
No. NAD+ is a dinucleotide coenzyme composed of nicotinamide- and adenine-containing nucleotide units joined through phosphate groups. It is included in the TalkingPeps peptide library because it is discussed and marketed alongside peptides.
What does the plus sign in NAD+ mean?
It denotes the oxidized redox form. NAD+ accepts reducing equivalents and becomes NADH; NADH can donate electrons and be oxidized back to NAD+. The symbol does not mean “extra-strength.”
Are NAD+, NADH, NMN, and NR interchangeable?
No. NADH is the reduced redox form, while NMN and NR are biosynthetic precursors. They differ in chemistry, absorption, metabolism, route, product status, and clinical evidence. A positive NR or NMN trial cannot be assumed to prove a direct NAD+ infusion effect.
Is IV NAD+ FDA approved?
There is no FDA-approved IV NAD+ product for anti-aging, energy, cognition, recovery, addiction treatment, or general wellness. NAD was listed in FDA’s May 2026 503A Category 1 nomination document as under evaluation; that category is not drug approval or final inclusion on a positive bulks list.
Does IV NAD+ reverse aging?
No direct human outcomes trial shows that IV or injected NAD+ slows, stops, or reverses aging, extends lifespan, reduces frailty, or prevents age-related disease. Cellular mechanism and blood biomarkers are not validated aging outcomes.
Does an infusion raise intracellular or mitochondrial NAD+?
That is not established across relevant human tissues. The 2019 pilot showed rapid disappearance from plasma early in infusion and later urinary metabolites, but it did not demonstrate delivery into brain, muscle mitochondria, or other target compartments.
What doses are discussed online?
Commercial discussions often mention 100–250 mg as an introductory amount, 500 mg as a common session, and 750–1,000 mg as a high-dose session. These are conventions, not validated wellness dosing. Direct disease trials have used much smaller 5–10 mg-class amounts in hospital contexts.
Why do some NAD+ infusions run slowly?
Commercial recipients commonly report cramping, nausea, chest pressure, faster heart rate, and other symptoms during infusion, and clinics may slow delivery for tolerability. Slower delivery is not proof of efficacy and cannot correct contamination, endotoxin, incorrect identity, or incompatibility.
Can NAD+ treat addiction or withdrawal?
Evidence is inadequate. Published case series used proprietary combinations, lacked placebo controls, and relied heavily on subjective before-and-after measures. NAD+ should not replace evidence-based withdrawal management or medications for substance-use disorders.
What do the heart-failure and hearing-loss trials prove?
They provide promising early, disease-specific signals from single-center studies. They do not prove anti-aging or wellness benefit, do not validate 500–1,000 mg commercial protocols, and require independent multicenter replication with clinically important endpoints.
Can NAD+ be stacked with glutathione, MOTS-c, or SS-31?
These combinations are discussed because all are linked to redox or mitochondrial narratives. No controlled human study establishes synergy, sequence, compatibility, combined safety, or better outcomes. Mixing products in one IV bag adds a separate compatibility and stability question.
Does a certificate of analysis prove an NAD+ vial is safe?
No. A useful certificate must be authentic, batch-specific, and supported by appropriate methods for identity, assay, impurities, microbial limits, and other attributes. Injectable finished products additionally require sterility, bacterial-endotoxin, particulate, container, stability, and release controls.
How should NAD+ be stored?
Use product-specific written instructions. Dry powder, concentrated injection, diluted infusion bag, oral supplement, salt form, excipients, container, and beyond-use period can all differ. Refrigeration is not a universal substitute for stability data.
What would stronger wellness evidence look like?
Independent randomized trials using a chemically defined and quality-controlled product, prespecified clinical outcomes, adequate blinding, verified tissue or cellular pharmacology, systematic adverse-event collection, meaningful follow-up, and transparent reporting of null as well as positive findings.
Where this information comes from
Explore related roadmap pages
Essential biology is not automatic treatment proof.
NAD+ is fundamental to cells, while direct wellness infusion benefits remain unproven and product quality can determine real-world risk.
Explore the Research Library