SS-31
Also called elamipretide, SS-31 is a synthetic mitochondria-targeted tetrapeptide. One prescription product now has a narrow accelerated FDA approval for Barth syndrome; that does not validate broad anti-aging, energy, recovery, or wellness use.
SS-31 at a glance
Designed to localize at mitochondrial membranes
SS-31 is not a hormone and does not copy a naturally circulating human peptide. Its alternating aromatic and positively charged residues allow it to associate with negatively charged mitochondrial membrane surfaces, especially cardiolipin-rich regions.
Membrane localization
Elamipretide partitions into the inner mitochondrial membrane interface. FDA describes it as a mitochondrial cardiolipin binder that localizes to the inner membrane.
Cardiolipin
Cardiolipin helps organize cristae and respiratory-chain complexes. Cell-free, cell, and animal studies show SS-31 can interact with cardiolipin and alter membrane electrostatics and packing.
Bioenergetics
Experimental work links SS-31–cardiolipin interactions to preserved cristae structure, electron transfer, oxygen consumption, and ATP recovery under stress. These are mechanistic observations, not proof of broad clinical benefit.
Oxidative injury
Preclinical models report less cardiolipin peroxidation, mitochondrial swelling, reactive oxygen signaling, and cell injury. Effects vary by model, timing, dose, and disease context.
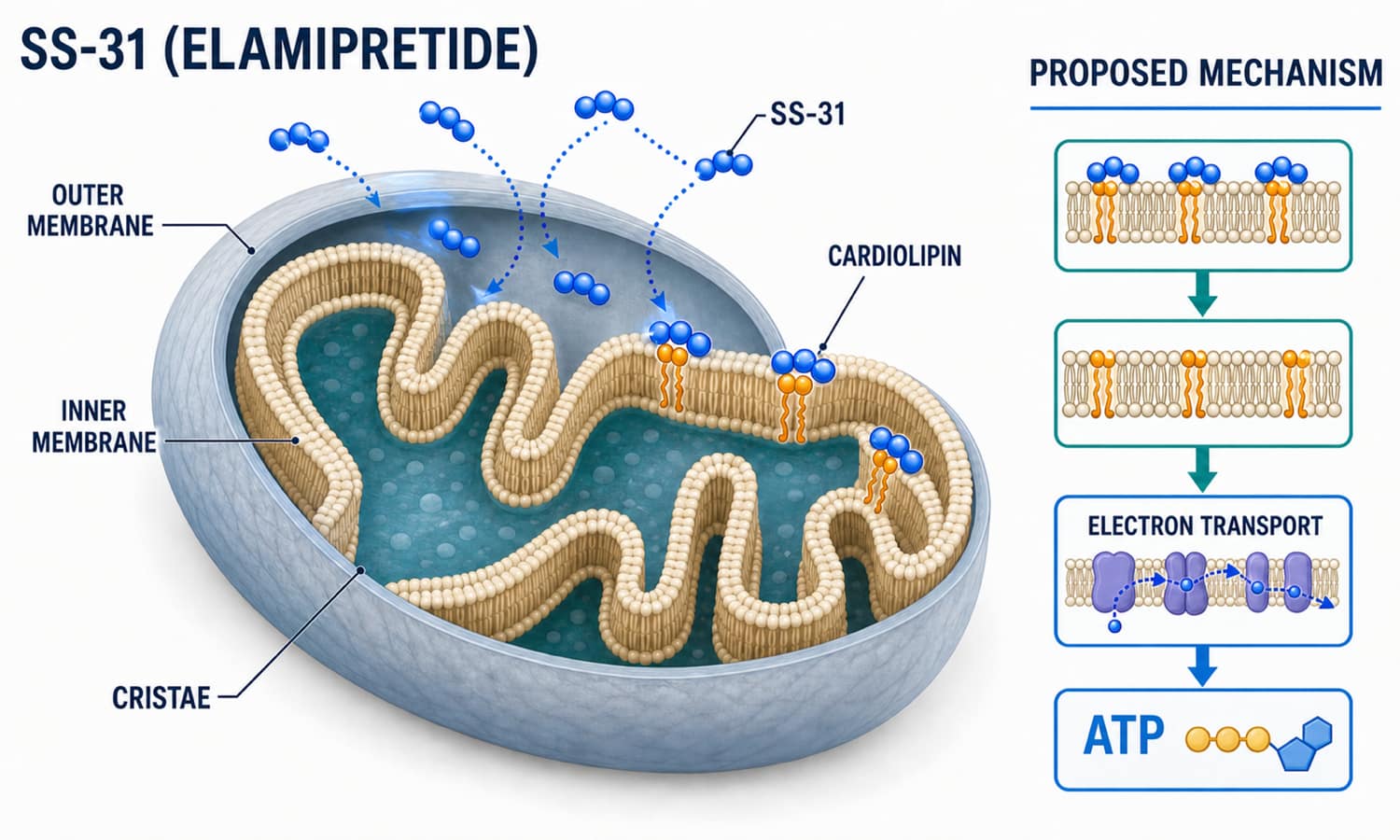
Planned image 1: SS-31–cardiolipin inner mitochondrial membrane mechanism map · 1500 × 900
What is reasonably established
- Elamipretide reaches peak concentration about 0.5–1 hour after subcutaneous dosing
- FDA labeling reports about 92% absolute subcutaneous bioavailability
- Exposure is dose-proportional from 2 to 80 mg with minimal accumulation
- Elamipretide and inactive peptide metabolites are primarily recovered in urine
- Renal impairment can substantially increase exposure
What the pathway does not prove
- That “supporting mitochondria” improves every condition involving mitochondrial stress
- That acute biomarker or imaging changes translate into daily function or longevity
- That lower community doses reproduce prescription-drug exposure
- That combining SS-31 with other mitochondrial compounds is synergistic
- That research-grade material matches Forzinity identity, formulation, purity, or sterility
A real clinical program—with important negative trials
Elamipretide has been administered to people in several diseases. That makes its evidence base far more developed than many research peptides, but results remain indication-specific and mixed.
| Program | Design and exposure | Main result | Evidence reading |
|---|---|---|---|
| FDA basis Barth syndrome / SPIBA-201 | 12 males, randomized crossover; 40 mg subcutaneous daily, followed by a small open-label extension | Not superior to placebo on randomized 6-minute walk or fatigue primary endpoints. Knee-extensor strength did not improve in the randomized period but increased descriptively during the open-label extension. | Accelerated approval relies on an intermediate endpoint in an ultra-rare disease. A confirmatory randomized trial is required. |
| Class I trial Primary mitochondrial myopathy / MMPOWER-3 | 218 participants; phase 3, randomized, double-blind; 40 mg daily for 24 weeks | Did not improve 6-minute walk distance or total fatigue versus placebo. | Strong evidence against a broad 24-week benefit for these two primary outcomes in this population. |
| Primary endpoints missed Dry AMD / ReCLAIM-2 | 176 participants; phase 2, randomized; 40 mg daily for 48 weeks | Primary visual-acuity and geographic-atrophy endpoints were not statistically significant. Exploratory ellipsoid-zone measures favored elamipretide. | Secondary or surrogate signals are hypothesis-generating; elamipretide is not FDA approved for AMD. |
| Small trial HFrEF / PROGRESS-HF | 71 participants; randomized; 4 mg or 40 mg daily for 28 days | No significant improvement in the primary left-ventricular end-systolic volume outcome. | Short duration and mechanistic rationale do not establish chronic heart-failure benefit. |
| Pilot evidence Renal artery stenosis | Phase 2a pilot around stent revascularization; intravenous peri-procedure use | Exploratory renal oxygenation, blood-flow, and kidney-function signals were reported. | Different route, timing, and clinical context; not a basis for home subcutaneous kidney protocols. |
| Preclinical Cells and animals | Numerous injury, aging, metabolic, cardiac, renal, muscle, and neurologic models | Often improved mitochondrial structure or stress responses. | Broad model success has not consistently translated to positive human primary endpoints. |
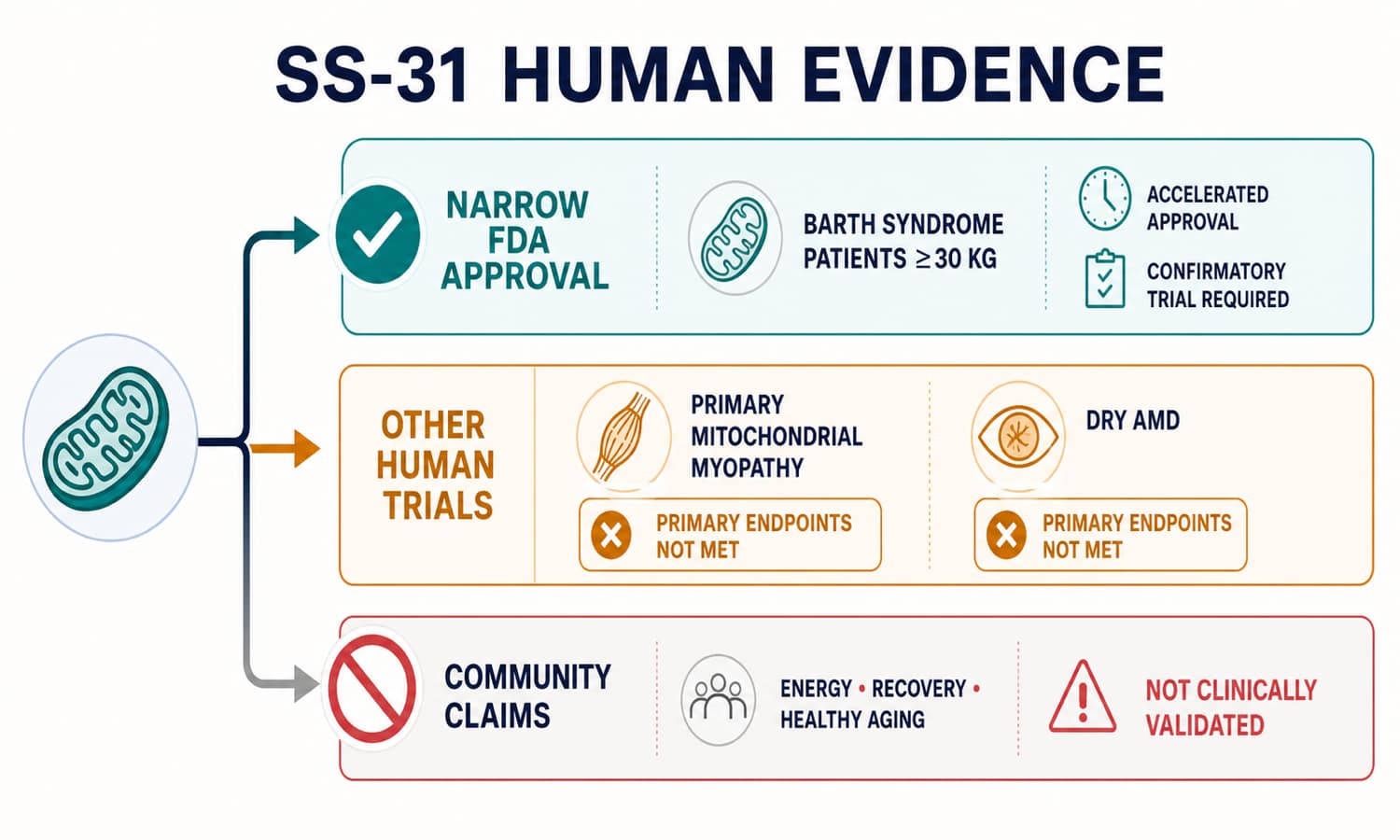
Planned image 2: SS-31 human evidence and regulatory boundary map · 1500 × 900
Forzinity is approved—but the approval is narrow and conditional
What is approved
- Forzinity (elamipretide) injection
- To improve muscle strength in adult and pediatric patients with genetically driven Barth syndrome
- Patients must weigh at least 30 kg
- 40 mg subcutaneously once daily for patients without severe renal impairment
- Approved September 19, 2025 through the accelerated approval pathway
Why “accelerated” matters
The approval was based on improvement in knee-extensor muscle strength, which FDA considers reasonably likely to predict meaningful patient benefit. The randomized part of the small supporting study did not show superiority on its primary walk or fatigue endpoints, and strength gains appeared during an open-label extension.
Continued approval may depend on a confirmatory randomized trial demonstrating clinical benefit.
What is not covered
The approved label does not cover generic fatigue, athletic performance, post-workout recovery, longevity, “mitochondrial optimization,” heart failure, kidney protection, primary mitochondrial myopathy, macular degeneration, neurodegeneration, or weight management. An approved active ingredient also does not make gray-market, compounded, or research products equivalent to the FDA-reviewed drug.
Common claims are much broader than the approved indication
What communities hope it does
- Raises energy, stamina, or exercise tolerance
- Improves recovery after intense training
- Reduces “mitochondrial oxidative stress”
- Supports healthy aging or cognitive resilience
- Protects heart, kidney, muscle, or nervous tissue
- Creates a “mitochondrial reset” before MOTS-c or NAD+ protocols
Evidence boundary
- Barth syndrome approval cannot be generalized to healthy adults
- MMPOWER-3 did not improve walk distance or fatigue
- ReCLAIM-2 missed both primary efficacy endpoints
- No controlled trials validate athletic, longevity, or stacking protocols
- Product identity and sterility can dominate real-world risk
- Subjective energy changes are highly vulnerable to expectancy and training changes
Community low-dose talk
Often discussed as an entry range or short “mitochondrial support” block. This is not an FDA-approved or clinically validated wellness regimen.
Community higher-dose talk
Sometimes used in short cycles or on training days. Human efficacy cannot be inferred from dose size, and cumulative injection-site exposure rises with daily use.
Clinical research context
Used in several development trials and in the approved Forzinity label for eligible Barth syndrome patients. It should not be copied into unsupervised protocols.
Common stacking conversations
| Stack discussion | Community rationale | Key limitation |
|---|---|---|
| SS-31 + MOTS-c | Pair membrane-focused mitochondrial support with a mitochondrial-derived metabolic signal | No controlled human combination study; elamipretide and MOTS-c have different evidence and regulatory status |
| SS-31 + NAD+ | Combine cardiolipin-focused biology with redox/cofactor-focused wellness protocols | No validated synergy, sequence, interaction advantage, or combined safety program |
| SS-31 + exercise | Attempt to support mitochondrial adaptation or recovery around endurance training | MMPOWER-3 did not improve the 6-minute walk endpoint; healthy-athlete benefit is untested |
| SS-31 + GLP-1 therapy | Try to offset fatigue during weight loss or calorie restriction | No established interaction or evidence that SS-31 treats medication-related fatigue; evaluate nutrition and medical causes first |
Mixing math for a hypothetical 10 mg vial
This section is arithmetic for understanding labels—not a preparation or dosing recommendation. It describes a hypothetical lyophilized 10 mg research vial with 2 mL final liquid. It does not describe Forzinity, which is supplied ready to use at 80 mg/mL and should not be reconstituted or mixed with another product.
| U-100 mark | Volume | Amount at 5 mg/mL | Calculation |
|---|---|---|---|
| 5 units | 0.05 mL | 0.25 mg (250 mcg) | 0.05 × 5 |
| 10 units | 0.10 mL | 0.50 mg (500 mcg) | 0.10 × 5 |
| 20 units | 0.20 mL | 1.00 mg | 0.20 × 5 |
| 40 units | 0.40 mL | 2.00 mg | 0.40 × 5 |
| 100 units | 1.00 mL | 5.00 mg | 1.00 × 5 |
Universal formula
Amount wanted ÷ concentration = volume.
Then convert volume to U-100 marks: mL × 100 = units. Example arithmetic: 1 mg ÷ 5 mg/mL = 0.20 mL = 20 units.
What causes errors
- Confusing elamipretide free-base amount with hydrochloride salt mass
- Copying an online table made for a different liquid volume
- Confusing 80 mg/mL prescription product with a 5 mg/mL example
- Using insulin syringe “units” as if they were milligrams
- Assuming a research vial is sterile or correctly labeled because the math works
Do not borrow the prescription label for a different product
Unopened Forzinity
FDA labeling says to refrigerate the ready-to-use vials at 2–8°C (36–46°F) and not freeze them. The sterile solution should be clear and colorless to yellow.
Opened Forzinity
After the first dose, the labeled vial may be kept refrigerated or at 20–25°C (68–77°F). The vial must be discarded eight days after first opening.
No same-syringe mixing
The FDA label directs users not to mix other products in the same syringe. It is single-patient-use and requires aseptic technique and daily site rotation.
Other SS-31 products
A lyophilized or compounded vial may have different salt form, excipients, concentration, sterility, and stability. Use its pharmacy or manufacturer documentation; do not assume Forzinity’s eight-day rule applies.
Human exposure data exist—and reveal practical risks
Injection reactions are not a footnote
In the 12-person Barth syndrome randomized crossover study, all elamipretide-treated participants had a local administration reaction. FDA lists erythema, pain, induration, itching, bruising, and urticaria. Injections are daily in the approved protocol, so site rotation and monitoring matter.
Serious hypersensitivity requiring emergency care has also occurred. Reactions may begin within minutes or only after months of treatment.
Stop and seek urgent help
- Trouble breathing, throat or facial swelling, widespread hives, faintness, or low blood pressure
- Rapidly spreading redness, severe pain, fever, drainage, or other signs of injection-site infection
- New confusion, severe weakness, presyncope, or persistent vomiting
- Any serious reaction after a new vial, concentration, or source
Higher-caution situations
- Known serious allergy to elamipretide or product excipients
- Kidney disease, especially eGFR below 30 mL/min or dialysis
- Pregnancy, breastfeeding, children below the labeled population, or older adults with limited trial representation
- Multiple injectable products or immunologic/skin disorders
- Use in tested sport or without a verified prescription supply chain
Common questions about SS-31
Are SS-31 and elamipretide the same thing?
SS-31 is the research name commonly used for elamipretide. Older literature may also use MTP-131 or Bendavia. Forzinity is the FDA-approved brand-name formulation of elamipretide.
Is SS-31 FDA approved?
Yes, elamipretide was approved as Forzinity on September 19, 2025. The accelerated approval is narrow: improving muscle strength in adults and children with Barth syndrome who weigh at least 30 kg. It is not a general approval for mitochondrial health or anti-aging.
What is Barth syndrome?
Barth syndrome is a rare, serious genetic mitochondrial disorder caused by TAZ gene variants and abnormal cardiolipin remodeling. It primarily affects males and can involve cardiomyopathy, muscle weakness, fatigue, exercise intolerance, neutropenia, and growth problems.
Why was approval accelerated?
FDA accepted improved knee-extensor muscle strength as an intermediate endpoint reasonably likely to predict benefit in an ultra-rare, life-threatening disease. A post-approval randomized trial must verify and describe clinical benefit.
Did the Barth syndrome trial meet its primary endpoints?
No. In the 12-person randomized crossover portion, elamipretide was not superior to placebo for the 6-minute walk test or fatigue primary endpoints. The muscle-strength signal supporting approval appeared descriptively during the open-label extension, not during randomized comparison.
Does SS-31 improve energy or exercise performance?
That is not established for healthy people. The 218-person MMPOWER-3 trial in primary mitochondrial myopathy did not improve 6-minute walk distance or total fatigue at 24 weeks. A narrow Barth syndrome approval should not be generalized to sports or wellness.
Does SS-31 work for eye disease?
ReCLAIM-2 in dry age-related macular degeneration missed its two primary efficacy endpoints. Some secondary ellipsoid-zone imaging and categorical vision findings favored elamipretide, supporting further research, but the drug is not FDA approved for AMD.
What doses are discussed online?
Community discussions often mention 4–5 mg or 10 mg daily in short blocks. These are not validated wellness protocols. Clinical development and the approved Barth label commonly use 40 mg daily of a specific pharmaceutical formulation; copying that dose to an unverified vial would be unsafe.
Can SS-31 be stacked with MOTS-c or NAD+?
People discuss these combinations because the compounds are associated with different parts of mitochondrial or metabolic biology. No controlled human trials establish synergy, dosing order, or combined safety.
Does Forzinity need reconstitution?
No. The FDA-approved product is a ready-to-use sterile solution supplied at 80 mg/mL. It should not be reconstituted, diluted based on internet mixing tables, or mixed with another product in the same syringe.
How long does SS-31 last in the body?
After subcutaneous administration, peak concentrations occur within about 0.5–1 hour and drug/metabolites are primarily eliminated in urine. A single “half-life” quoted online is less useful than the full labeled pharmacokinetic context, especially because kidney impairment increases exposure.
Is a research vial equivalent to Forzinity?
No. The approved product has reviewed identity, salt form, concentration, excipients, manufacturing, sterility, stability, labeling, and pharmacovigilance. A vial labeled SS-31 may not match any of those attributes.
Where this information comes from
Explore related roadmap pages
Separate target biology from treatment proof.
SS-31 has a credible mitochondrial target and a real approval—but only one narrow accelerated-approval indication.
Explore the Research Library