BPC-157 + TB-500
This popular “recovery stack” combines two different investigational peptides. The repair story is compelling online, but controlled human evidence for the combination is almost nonexistent.
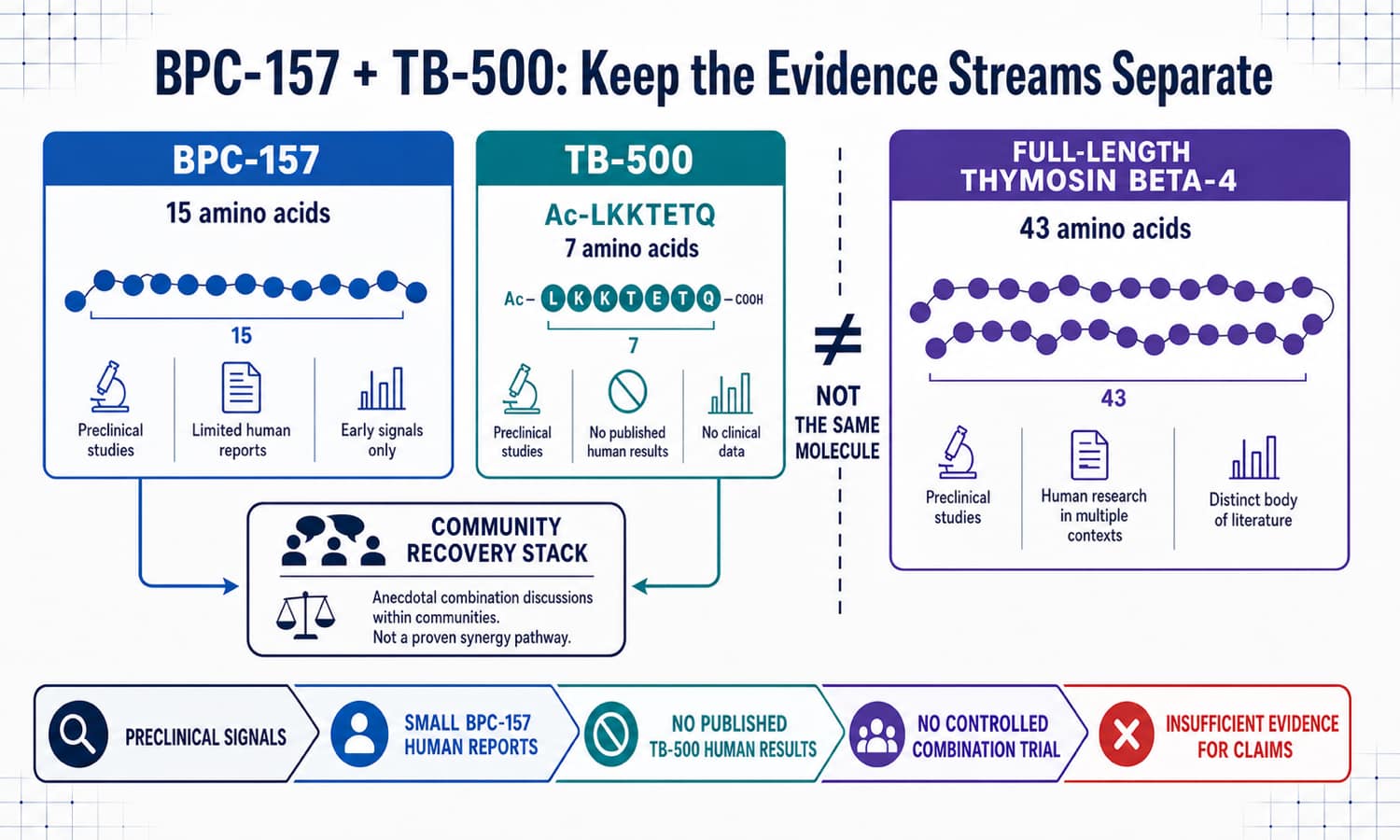
Three evidence streams are often blurred together
The combination makes sense to users because both peptides are associated with repair biology. But BPC-157, TB-500 and full-length thymosin beta-4 must be evaluated separately.
A blend is not a formulation
The label still needs exact forms, amount of each component, sterility, endotoxin control, compatibility and stability.
“Near the injury” is unproven
No controlled evidence shows that local injection improves delivery or outcome, and anatomy-specific injection risks remain.
Anecdotes mix variables
Time, reduced training, rehabilitation, sleep, nutrition, placebo and other drugs can all look like a peptide effect.
The combination has almost no clinical evidence
Small BPC-157 reports, animal experiments, full-length Tβ4 work and community recovery stories do not add up to a controlled trial of BPC-157 plus TB-500.
Very limited human reports
Human evidence is short, small and spread across different routes and conditions. It does not validate a subcutaneous tendon, ligament or muscle-recovery protocol.
No published human results
FDA's review found no human exposure studies. A recruiting registry study is planned research, not evidence of safety or recovery benefit.
Four uncontrolled patients
A knee chart review included only four people receiving BPC-157 plus a product reported as TB4. There was no placebo, imaging or verified TB-500 identity.
What would test synergy
- BPC alone, TB-500 alone, combination and placebo
- Verified molecules and a stable formulation
- Standard rehabilitation across all groups
- Function, imaging and return-to-activity endpoints
What remains unknown
- Human TB-500 pharmacokinetics and safety
- An effective dose or combination ratio
- Whether local injection changes delivery
- Whether either peptide reduces reinjury
How the “Wolverine stack” is commonly used
These patterns describe recurring internet practice. They are not approved doses, validated protocols or evidence that a fixed blend improves recovery.
BPC-157 pattern
Users commonly describe daily or divided use for two to six weeks, sometimes “near the injury.” Human pharmacokinetics and a recovery dose are not established.
TB-500 pattern
Community protocols describe several “loading” weeks followed by less-frequent maintenance. No human trial validates either phase.
Premixed blend
Equal mass is a sales format, not a proven biological ratio. A fixed blend prevents independent adjustment and makes reactions harder to attribute.
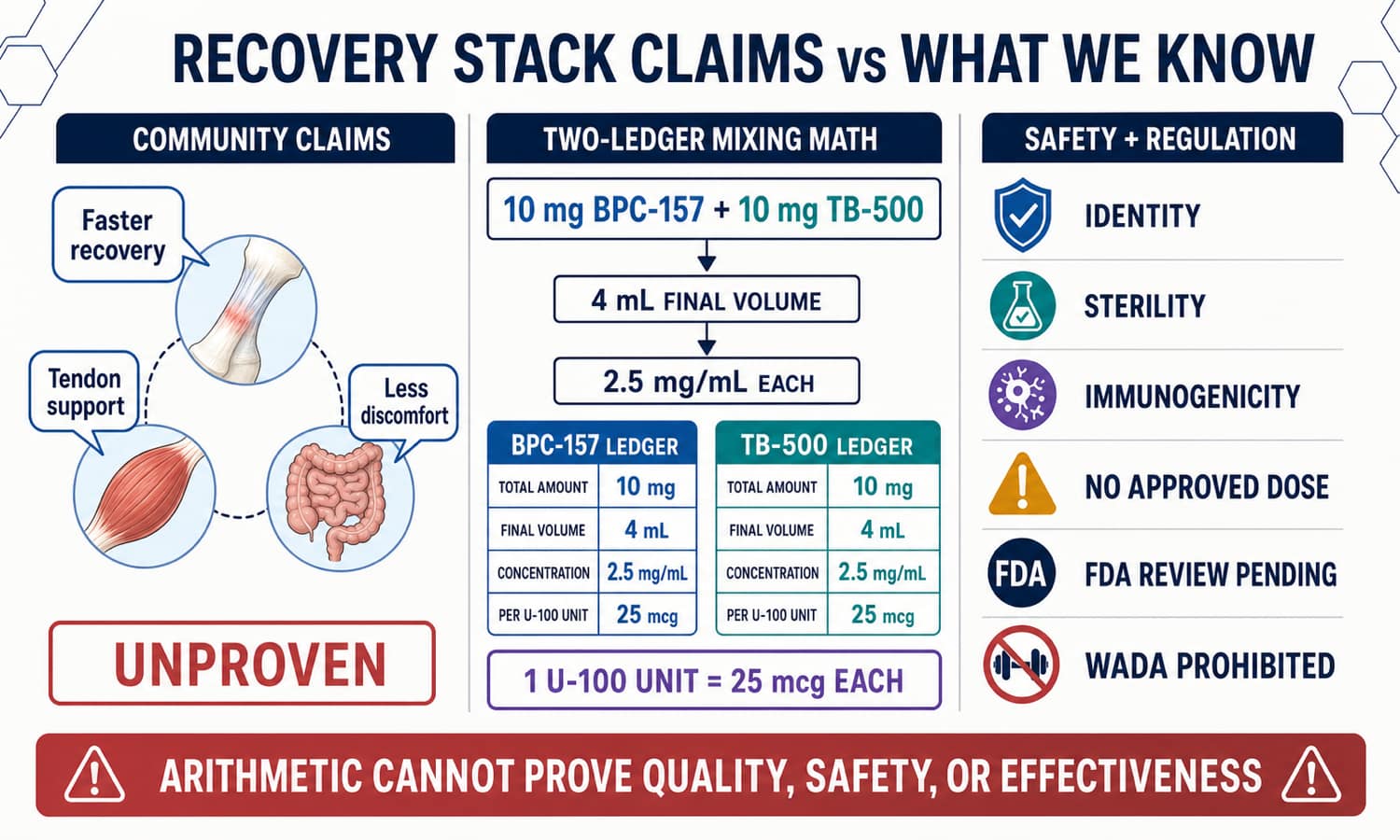
A blend needs two separate concentration ledgers
Worked arithmetic—not dosing advice
If a hypothetical vial claims 10 mg BPC-157 plus 10 mg TB-500 and the verified final volume is 4 mL, each peptide calculates to 2.5 mg/mL.
What math cannot answer
- Whether both labeled peptides are present
- Whether mass means free base or salt
- Whether both dissolve uniformly and remain compatible
- Whether the product is sterile or stable
- Whether any calculated amount is safe or effective
No universal mixed shelf life
Raw-powder freezer claims do not establish stability for a reconstituted, multi-dose blend. Follow a legitimate pharmacy's product-specific label.
Sterility is invisible
Clear liquid and bacteriostatic water cannot rule out contamination, endotoxin, particles or a damaged container.
Two unknown safety profiles
Starting both together makes allergy, rash, pain, laboratory changes or other reactions harder to attribute.
Important uncertainty
- Long-term immune and aggregation risk
- Effects in active cancer or abnormal vascular disease
- Pregnancy, reproductive and developmental safety
- Injection injury near tendon, nerve, vessel or joint
- Unknown product identity or sterility
Seek urgent care for
- Trouble breathing, facial swelling, hives or fainting
- Chest pain or new neurologic symptoms
- Rapidly spreading redness, severe joint pain or pus
- Fever, confusion or signs of bloodstream infection
BPC-157 and TB-500 FAQs
Are they the same peptide?
No. BPC-157 has 15 amino acids; TB-500 is a seven-amino-acid acetylated fragment.
Is TB-500 thymosin beta-4?
No. Full-length Tβ4 contains 43 amino acids. Its evidence cannot automatically be transferred to TB-500.
Is the combination FDA-approved?
No. There is no FDA-approved BPC-157/TB-500 medicine, indication, dose or combination label.
Has the stack had a randomized trial?
No controlled randomized combination trial was identified. The tiny knee subgroup was uncontrolled and used a product described as TB4.
Does injection near an injury work better?
No controlled evidence establishes that it does. Local injection can add nerve, vessel, tendon and joint risks.
What does “loading” mean?
It is community language for larger or more frequent early TB-500 exposure, not a validated human protocol.
Research behind this page
Related roadmap pages
Two repair stories do not make one proven treatment.
BPC-157 and TB-500 have different identities, unequal evidence and no validated recovery-stack protocol.
Explore the Research Library