Beginner guide
Understanding Placebo-Controlled Trials
A placebo helps build a fair comparison. It lets researchers estimate what changed because of the test intervention—and what might have changed anyway.
A placebo-controlled trial asks: what extra difference did the intervention make?
Participants are assigned to a test group or a matched placebo group, usually by chance. Both groups share the visits, attention, expectations, measurements, and passage of time. The planned difference is the active intervention. Researchers compare outcomes between groups; improvement in the test group by itself is not enough.
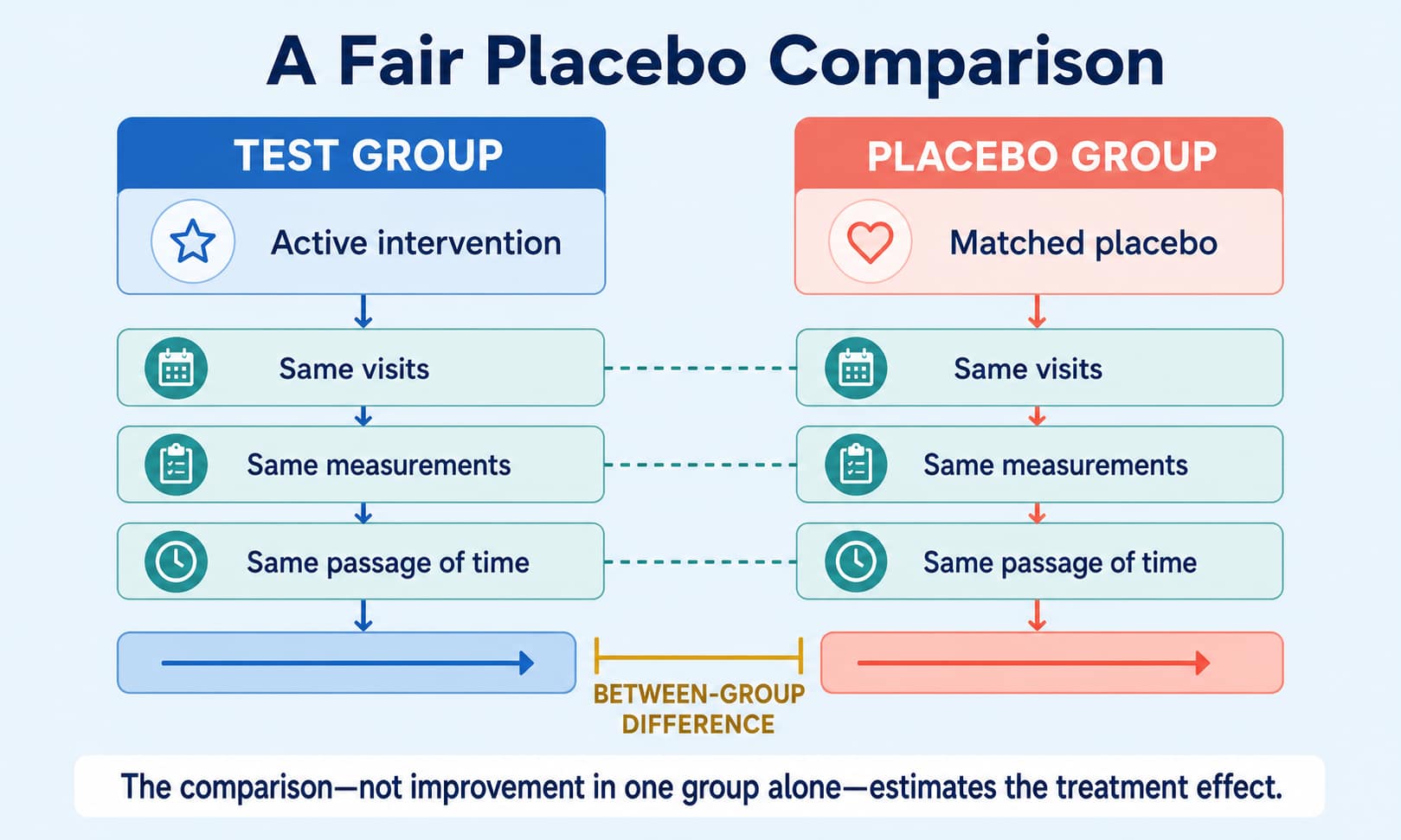
One planned difference
A placebo makes one difference easier to see
A placebo is an inactive substance or treatment designed to resemble the intervention and be given in the same way. It may be a tablet, liquid, injection, or sham procedure. Its ingredients, route, timing, and surrounding care still need to be described.
The whole trial package
Active intervention plus scheduled visits, instructions, allowed background care, expectations, measurements, and time.
- Receives the test intervention
- Follows the written protocol
- Reports outcomes and adverse events
The matched trial package
Matched placebo plus the same planned visits, instructions, allowed background care, expectations, measurements, and time.
- Does not receive the active component
- Follows the same protocol
- Reports the same outcomes and adverse events
A useful distinction
“Placebo response” is a basket, not one effect
People often call every improvement in the placebo group “the placebo effect.” That is too simple. The observed change can contain several different influences.
Natural course
Symptoms may improve, fluctuate, or worsen over time without the active intervention.
Regression to the mean
People often enter a trial when symptoms are unusually high; later readings may move closer to their usual level.
Expectations and context
Anticipation, attention, routines, and interactions can affect some reported experiences.
Other care
Allowed background treatment, rest, behavior changes, or rescue medicine may influence outcomes.
Measurement
Day-to-day variability, learning a test, reporting, and measurement error can move scores.
Chance and missing data
Small samples, dropouts, and random variation can make the observed change unstable.
Three locks on a fair test
A placebo alone does not prevent bias
The label “placebo-controlled” tells you the comparator. It does not tell you whether group assignment, blinding, follow-up, or analysis were handled well.
Randomization
Assignment by chance helps prevent known and unknown baseline differences from being systematically packed into one group. Check how the random sequence was generated and concealed until assignment.
Matching and blinding
The placebo should resemble the test intervention in relevant ways. Ask exactly who was unaware of assignment: participants, care providers, investigators, outcome assessors, or analysts.
Equal handling
Visits, instructions, background care, outcome timing, encouragement, rescue rules, and follow-up should be comparable. Dropouts and harms should be reported for each group.
A fictional result
Read the gap, not just the dramatic change
This arithmetic is only a study-reading example. It uses a fictional intervention and no dosing or treatment instructions.
The comparator must fit the question
A placebo is useful, but not always the right control
Control groups are design choices. Researchers may need to learn whether something works at all, whether it adds benefit, or how it compares with established care.
Placebo control
Useful for estimating whether the intervention has an effect beyond the matched trial experience, especially when no proven effective intervention must be withheld.
Active control
Compares the new intervention with an established treatment. The question may be superiority or whether the new option is not unacceptably worse under a prespecified margin.
Add-on design
Both groups receive background standard care; one adds the test intervention and the other adds placebo. This can preserve care while isolating the added component.
A six-question reader screen
Before trusting the conclusion, find these answers
A trial report or registry record should let you identify the comparison without guessing.
Who was randomized?
Check eligibility, sample size, baseline features, setting, and whether the population fits the headline.
What exactly was the placebo?
Look for ingredients or procedure, route, timing, appearance, and allowed background care.
Who was blinded?
Prefer named roles and methods over an unexplained “single-” or “double-blind” label.
What was the primary outcome?
Find the prespecified measure, time point, and whether lower or higher values mean improvement.
What was the between-group result?
Read the effect estimate and confidence interval, not only each group’s change or a p-value.
What happened to safety and follow-up?
Compare adverse events, rescue treatment, adherence, withdrawals, missing data, and analysis counts.
Quick answers
Placebo-controlled trials: FAQs
Does placebo mean participants receive no care?
Not necessarily. Both groups may receive standard care, monitoring, or rescue treatment. The placebo replaces only the controlled component; check the protocol.
Is a placebo always a sugar pill?
No. It can be a matched tablet, liquid, injection, device, procedure, or attention control designed to support the intended comparison.
If both groups improve, did the intervention fail?
Not automatically. The question is usually whether the groups differ meaningfully, considering the estimate, uncertainty, harms, and planned analysis.
Does “no significant difference” prove the treatments are equal?
No. The trial may be imprecise or unable to detect a difference. Equivalence and non-inferiority need specific designs, margins, and analyses planned in advance.
Can a placebo-controlled trial prove an intervention is safe?
No. It can compare observed adverse events, but limited size or follow-up may miss uncommon, delayed, or population-specific harms.
Keep learning