Comprehensive Metabolic Panel Explained
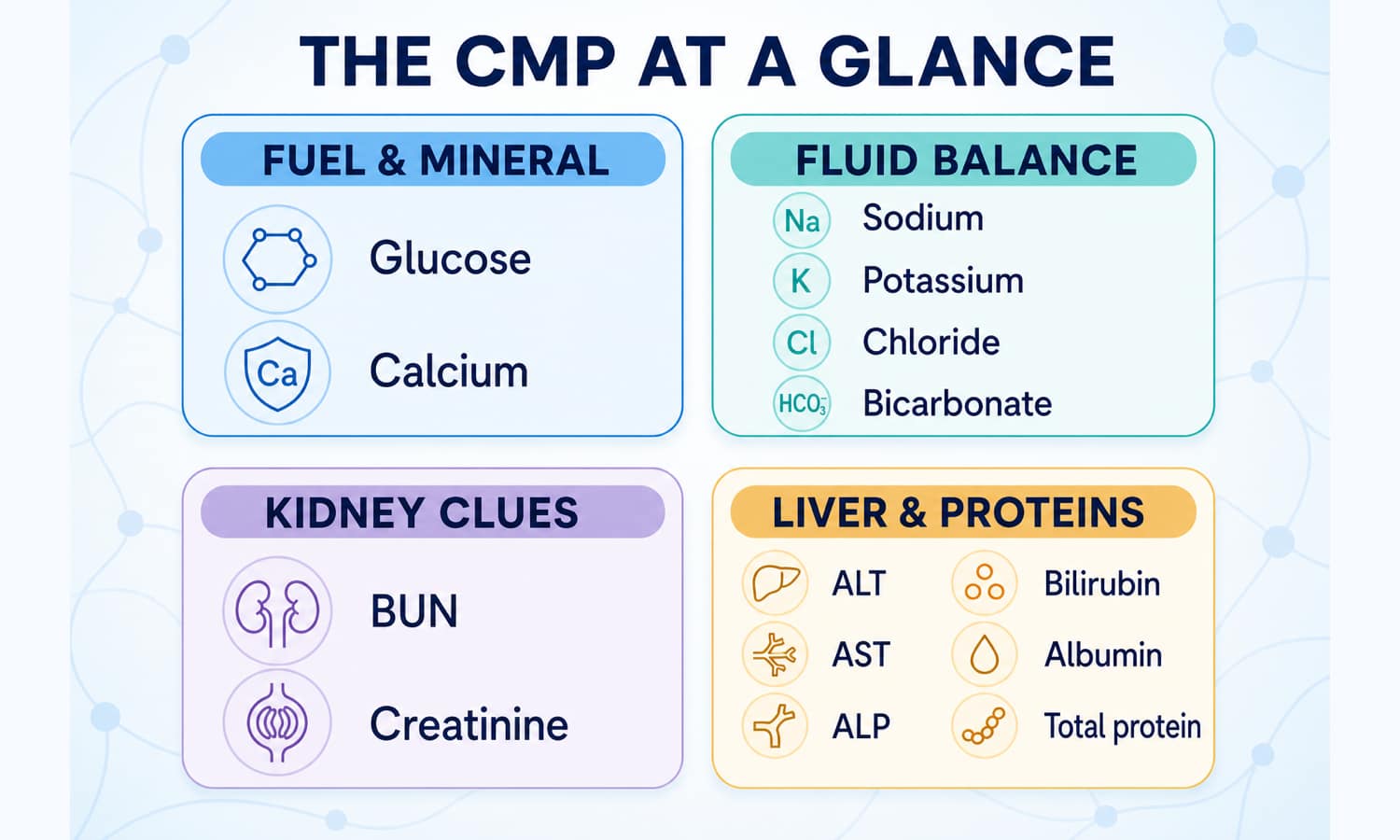
A CMP is 14 measurements in one blood draw. Together they offer a broad snapshot of blood sugar, fluid and electrolyte balance, kidney filtration clues, and liver- and protein-related patterns.
Think “four questions,” not “14 diagnoses.” A flagged value is a clue. Its size, neighboring results, symptoms, preparation and trend determine what it may mean.
Four questions inside one panel
A standard CMP usually contains the same 14 measurements. No single group gives a complete diagnosis.
What is circulating right now?
Glucose is a moment-in-time blood sugar measurement. Blood calcium supports nerve, muscle and heart function; it does not measure bone calcium stores.
Context: meals, fasting instructions, illness, medicines and albumin can matter.
Are electrolytes moving together?
These charged minerals help regulate fluid, acid-base balance, nerves and muscles. Vomiting, diarrhea, heavy sweating, kidney problems and some medicines can shift the pattern.
Context: a sample problem can sometimes distort a result—especially potassium.
How are waste markers being handled?
BUN and creatinine are waste-related measurements used alongside an estimated filtration rate (eGFR). Muscle size, meat intake, creatine use and hard training can affect creatinine.
A CMP does not include urine albumin, a separate kidney test used in many situations.
Is there a pattern of injury, flow or protein change?
ALT, AST and ALP are enzymes; bilirubin is a breakdown product; albumin and total protein add context. AST also comes from muscle, and ALP can come from bone, so the pattern matters.
An enzyme flag alone does not show cause or permanent damage.
High and low are starting points, not conclusions
Use your report’s own range. Laboratories may use different methods and intervals, and age, sex, pregnancy and clinical circumstances may change interpretation.
When something is high
- Concentration can matter: fluid loss may raise BUN, albumin or total protein without creating more of those substances.
- Source can matter: AST may rise after muscle injury; ALP may reflect liver or bone.
- Clearance can matter: creatinine or potassium may rise when kidney handling changes, but medicines and the test sample also deserve review.
When something is low
- Loss or dilution can matter: vomiting, diarrhea, excess fluid or some medicines may affect electrolytes.
- Intake is only one possibility: a low protein-related result is not automatically proof of a poor diet.
- Relationships matter: calcium is often interpreted with albumin; bicarbonate with the other electrolytes and clinical setting.
Reconstruct the day around the draw
CMP values are sensitive to what entered, left or stressed the body. A short test note can prevent a temporary influence from being mistaken for a stable trend.
Do not stop prescriptions to create a “cleaner” result unless your clinician directs it.
Was fasting requested? Note the draw time, recent meals, alcohol and whether you followed the laboratory’s instructions.
Record vomiting, diarrhea, heavy sweating, poor intake and unusual thirst. These can change electrolytes and concentration-sensitive results.
Strenuous exercise can temporarily shift AST, ALT, creatinine and other measurements. Note an unusually hard session or muscle injury.
List prescriptions, over-the-counter products, hormones, creatine and research compounds with timing. This is context for a clinician—not a cue to self-adjust.
Retesting after an unusual week can be sensible—with limits
Training, GLP-1, peptide and weight-loss communities often compare CMPs during dehydration, rapid weight change or heavy training. That habit can clarify noise when it stays connected to medical context.
Log fluids, meals and training
They repeat an unexpected panel under more typical conditions and compare creatinine, BUN, electrolytes and liver-related markers together.
The setup affects several values
Fluid loss, under-eating, vomiting and intense exercise can create coordinated short-term shifts, especially during rapid weight loss or demanding training.
“It is just dehydration” is not proof
Persistent abnormalities, medication effects and organ disease can look similar. Rehydrating or resting should not replace timely evaluation of symptoms or major changes.
A practical next-step path
Most unexpected CMP results need a better question, not a home treatment plan.
Check the context
Confirm units, your laboratory range, preparation, symptoms, fluid loss, exercise, medicines and supplements.
Look at the pattern
Compare prior CMPs and related values. Ask whether the change is isolated, coordinated, persistent or moving quickly.
Discuss what would clarify it
Ask whether repeat testing, eGFR, urine albumin, a focused liver panel or another targeted test fits your situation.
Quick questions
Do I need to fast for a CMP?
Sometimes. A CMP includes glucose, but preparation depends on why the panel was ordered and what other tests share the draw. Follow the exact instructions from your clinician or laboratory rather than fasting automatically.
Does a normal CMP prove my liver and kidneys are healthy?
No. It is a broad screen. Kidney assessment may also use eGFR and urine albumin, while liver concerns may require history, examination, focused blood tests or imaging. Symptoms and risk factors still matter.
What is the difference between a CMP and a BMP?
A BMP usually covers glucose, calcium, electrolytes, BUN and creatinine. A CMP adds albumin, total protein, ALT, AST, ALP and bilirubin.
Could hard training make liver markers look abnormal?
It can temporarily raise AST and sometimes ALT because exercise stresses muscle and changes body fluids. That possibility is context, not a diagnosis; persistent or substantial elevations still need proper evaluation.
Should I correct a flagged electrolyte with supplements?
Not on the basis of one result. Potassium and sodium problems can be dangerous, and the cause determines the response. Contact a clinician for unexpected results, especially when symptoms or a major abnormality are present.